
Page 159 - tmp
P. 159
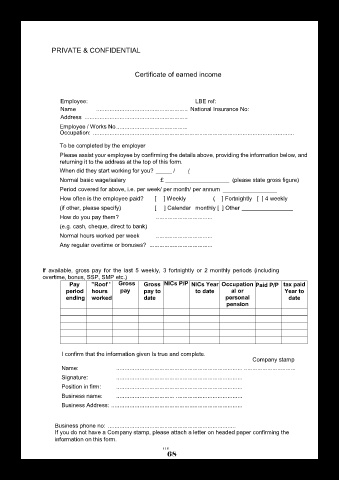
PRIVATE & CONFIDENTIAL
Certificate of earned income
Employee: LBE ref:
Name ....................................................... National Insurance No:
Address ..............................................................
Employee / Works No...........................................
Occupation: .........................................................................................................................
To be completed by the employer
Please assist your employee by confirming the details above, providing the information below, and
returning it to the address at the top of this form.
When did they start working for you? _____ / /
Normal basic wage/salary £ ____________________ (please state gross figure)
Period covered for above, i.e. per week/ per month/ per annum _________________
How often is the employee paid? [ ] Weekly ( ] Fortnightly [ ] 4 weekly
(if other, please specify) [ ] Calendar monthly [ ] Other ________________
How do you pay them? ..................................
(e.g. cash, cheque, direct to bank)
Normal hours worked per week ..................................
Any regular overtime or bonuses? ......................................
If available, gross pay for the last 5 weekly, 3 fortnightly or 2 monthly periods (including
overtime, bonus, SSP, SMP etc.)
Pay "Roof ' Gross Gross NICs P/P NICs Year Occupation Paid P/P tax paid
period hours pay pay to to date al or Year to
ending worked date personal date
pension
I confirm that the information given Is true and complete.
Company stamp
Name: ............................................................................ ...............................
Signature: ............................................................................
Position in firm: ............................................................................
Business name: ................................... ........................................
Business Address: ...............................................................................
Business phone no: .............................................................................
If you do not have a Company stamp, please attach a letter on headed paper confirming the
information on this form.
r\ r
68